
Ammar Al Mousa, BCPS; Abir T. El-Alfy, PhD, MS
WMJ. 2026;125:P2. Published online June 10, 2026.
Myqorzo was approved on December 19, 2025, based on the results of the SEQUOIA-HCM trial for the treatment of adults with symptomatic obstructive hypertrophic cardiomyopathy (oHCM) to improve functional capacity and symptoms.
MECHANISM OF ACTION
Myqorzo is a second‑in‑class, selective, oral, reversible cardiac myosin inhibitor that binds an allosteric pocket on the myosin motor domain, slowing phosphate release and preventing transition to the strong actin‑binding, force‑generating state. By stabilizing myosin in a low‑activity conformation and reducing the number of active actin myosin cross‑bridges within the cardiac sarcomere, aficamten decreases left ventricular contractility, mitigates hypercontractility in hypertrophic cardiomyopathy, and lowers left ventricular outflow tract (LVOT) obstruction.
Compared with mavacamten, the first cardiac myosin inhibitor, aficamten was developed to exhibit a more gradual dose-response relationship and a shorter half-life (~80 hours vs 6-9 days for mavacamten), thereby permitting dose titration at 2-week interval.
CLINICAL TRIAL DATA
SEQUOIA-HCM Trial
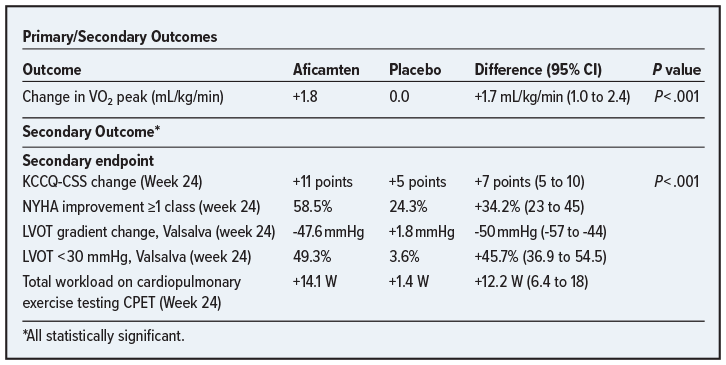
The SEQUOIA-HCM is a phase 3, double‑blind, randomized clinical trial that assessed the safety and effectiveness of aficamten . In this trial, adults with symptomatic obstructive hypertrophic cardiomyopathy were assigned to receive aficamten or placebo for 24 weeks, with dose titration to a maximum of 20 mg per day guided by echocardiographic assessment. Patients (N=282) were randomized: 142 received aficamten and 140 received a placebo. The primary endpoint was the change in peak oxygen uptake (peak VO2) from baseline to week 24, which demonstrated a clinically meaningful improvement with aficamten. All 10 prespecified secondary endpoints favored aficamten, including a 7‑point improvement in the Kansas City Cardiomyopathy Questionnaire – Clinical Summary Score (KCCQ-CSS) and an improvement in the New York Heart Association (NYHA) class. No difference was observed in the incidence of serious adverse events between groups: serious adverse events were reported in 8 patients (5.6%) in the aficamten group and in 13 patients (9.3%) in the placebo group. Reductions in left ventricular ejection fraction (LVEF) to <50% did not require treatment interruption and were not associated with clinical heart failure.
 At week 12, aficamten demonstrated significant improvements across all prespecified endpoints, including KCCQ‑CSS, NYHA class, LVOT gradient reduction, and achieving LVOT <30 mmHg, mirroring the direction and consistency of the week‑24 findings. Additionally, aficamten markedly reduced the duration of eligibility for septal reduction therapy by 78 days (95% CI, -100 to -56), reflecting rapid hemodynamic improvement and reduced procedural need. A rapid onset of effect was also noted. The LVOT gradient reduction was seen as early as 2 weeks.
At week 12, aficamten demonstrated significant improvements across all prespecified endpoints, including KCCQ‑CSS, NYHA class, LVOT gradient reduction, and achieving LVOT <30 mmHg, mirroring the direction and consistency of the week‑24 findings. Additionally, aficamten markedly reduced the duration of eligibility for septal reduction therapy by 78 days (95% CI, -100 to -56), reflecting rapid hemodynamic improvement and reduced procedural need. A rapid onset of effect was also noted. The LVOT gradient reduction was seen as early as 2 weeks.
DOSAGE AND ADMINISTRATION
- Start: 5 mg orally once daily with or without food
- Available strengths: 5 mg, 10 mg, 15 mg, 20 mg
- Titrate: Increase by 5 mg every 2 to 8 weeks
- Maximum dose: 20 mg daily
- Individualized based on LVEF and LVOT gradient
Cost
- All strengths: $356.38 per tablet (5 mg, 10 mg, 15 mg, and 20 mg all priced identically)
ADVERSE EFFECTS
- Hypertension
- LVEF reduction
- New or worsening chest pain
CONTRAINDICATIONS
- Concomitant rifampin (strong CYP3A/CYP2C19 inducer)
Do NOT initiate if LVEF <55%. Interrupt therapy if LVEF <40%.
CRITICAL MONITORING REQUIREMENTS
- Myqorzo is dispensed exclusively through a Risk Evaluation and Mitigation Strategy due to a boxed warning for the potential for systolic dysfunction and heart failure
- Echocardiogram assessments of LVEF are required before and during use.
DRUG/FOOD INTERACTIONS
Myqorzo is metabolized primarily by CYP2C9, with contributions from CYP3A4, CYP2D6, CYP2C19.
- Rifampin induces CYP3A4, CYP2C19, and CYP2C9 enzymes, thus may decrease aficamten levels and effectiveness. Dose adjustments are required when starting or stopping these agents. Similarly, other strong CYP3A4 inducers may decrease serum levels of aficamten.
- Strong CYP2C9 inhibitors (eg, fluconazole and voriconazole) and CYP2C19 inhibitors (eg, fluvoxamine) may raise aficamten levels, potentially increasing the risk of heart failure.
CONCLUSIONS
The approval of Myqorz (aficamten) represents a significant advancement in the treatment of symptomatic obstructive hypertrophic cardiomyopathy and introduces a targeted mechanism of action that directly addresses cardiac hypercontractility. Participants in the SEQUOIA‑HCM trial demonstrated meaningful improvements in exercise capacity, symptoms, and quality of life, along with substantial reductions in LVOT gradients. Additionally, aficamten offers a distinct safety and monitoring profile compared with existing therapies, with reversible reductions in ejection fraction and hypertension as the most notable adverse effects. Due to its mechanism as a cardiac myosin inhibitor, aficamten may reduce the need for invasive septal reduction therapy in appropriate patients. Ultimately, Myqorzo provides an important therapeutic option for patients who remain symptomatic despite guideline‑directed medical therapy or who are not ideal candidates for procedural intervention. From an accessibility standpoint, the manufacturer’s pricing remains high, and insurance coverage will play a key role in determining real‑world availability for patients.